Restoring Confidence with Natural and Symmetrical Results
Inverted nipple correction
The Impact of Inverted Nipples on Aesthetic and Physical Well-Being
DEFINITION AND RELEVANCE OF THE PROBLEM
Inverted nipples are relatively common condition, affecting approximatly 2% of the female population, according to scientific literature. This condition can lead to various issues, including poor hygiene in the areola area, breastfeeding difficulties, psychological distress, dissatisfaction with appearance and reccuring nipple inflamation. Most cases are congenital and may be linked to a genetic predispotion. Acquired nipple inversion typically results from chronic inflammation, cancer, macromastia, or prior surgical procedures. Factors influencing nipple inversion include insufficient supporting tissues, underdeveloped lactiferous ducts, and retraction caused by fibous bands at the base of the nipple.
Types of Inverted Nipples and Their Surgical Solutions
CLASSIFICATION
Physicians commonly use a classification system based on the effort requires. To manually evert the nipple, the duration od nipple protrusion, and the level of fibosis around the nipple.
In Grade I inversion , the nipple cam be easily pulled out manually and maintains its projection relativly well. These nipples exhibit minimal fibrosis.
Grade II inversion is the most common, where the nipple can be pulled out but does not maintain projection and tends to retract. These nipples have moderate fibrosis beneath them.
In grade I inversion the nipple is easily pulled out manually and maintains its projection quite well. Grade 1 nipples have minimal fibrosis.
In Grade III inversion, the nipple is difficult to pull out manually due to severe fibrosis.
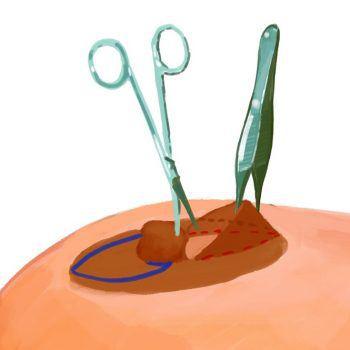
OPERATION
Inverted nipple correction istypically performed under local anaesthesia, though general anasthesia may be used for more complex procedures.
For Grade I inversion , manual traction combined with a single buried purse-string suture 5 mm incisions at the nipple base is usually sufficient.
In Grade II inversion ,surgical dissection is carried out until the nipple maintains its projection after releasing the traction. A purse-string suture is then employed to secure the nipple’s shape.
For Grade III inversion, precise surgical dissection of fibrotic fibers is performed while preserving the lactiferous ducts. Dermofibrotic or sub-dermal flaps are created to fill the area beneath the nipple, providing a foundation to maintain nipple protrusion.
These techniques aim to correct nipple inversion effectivly, with choice of method tailored to severity of the condition.
Post-Operative Care and Risks
Inverted Nipple Correction Surgery
POST-OPERATIVE PERIOD
Usually healing process typically takes about two weeks. After surgery, the nipple is secured with a shape-preserving bandage, and the dressing is changed every 2-3 days. Skin stitches are usually removed 10 days post-surgery. While the final aesthetic result becomes apparent after 2-3 months, changes in shape are not noticeable immediately after the procedure. The effects of the operation are long-lasting.
OPERATIONAL RISK
As with any surgery inverted nipple correction may have adverse effects: reaction to the anesthesia, bleeding, wound infection, nipple deformity and sensory disorders, scar hypertrophy. Operational risk is discussed during the consultation.
PRICES
Nipple correction (recessed nipple correction) from 700 €